Cirrhosis
Key points
- Many things can affect the health of the liver and lead to long-term liver damage
- Cirrhosis is the result of long-term liver damage
- Cirrhosis means scarring of the liver
- The liver shrinks and becomes hard and lumpy
- It can cause serious health problems
- Fixing the underlying problem can stabilise disease, ensure the liver is still able to function properly, slow or stop progression, and prevent complications like liver failure
- It’s never too late to make a change
Get your guide with everything you need to know about living with cirrhosis
Click on the picture below to download our booklet that gives you all the latest advice, written by trusted, clinician experts, on understanding cirrhosis.
What is cirrhosis?
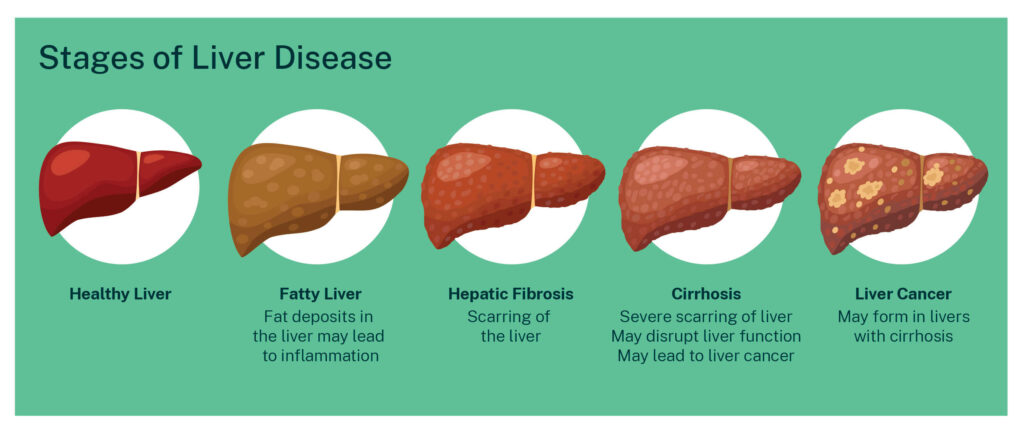
Cirrhosis means scarring of the liver. It is the result of long-term liver damage.
A healthy liver is soft and smooth. But when something damages the liver, scar tissue begins to form. This scarring is called fibrosis. It happens little by little over many years.
When the entire liver is scarred, it shrinks and gets hard and lumpy. This is called cirrhosis. Any long-term condition that damages the liver may lead to fibrosis and, eventually, cirrhosis.
A liver with cirrhosis can have problems getting all its work done, such as producing substances to clot the blood, digesting sugar and vitamins, or getting rid of toxins and bacteria. Liver cancer can also develop in a liver with cirrhosis.
It is estimated that cirrhosis affects at least 1 in 200 Australians.
What are the symptoms and stages of cirrhosis?
 At first, while the liver is functioning normally, you may have no symptoms at all. This is called compensated cirrhosis.
At first, while the liver is functioning normally, you may have no symptoms at all. This is called compensated cirrhosis.
As cirrhosis gets worse, you can develop major complications. This is called decompensated cirrhosis.
Compensated cirrhosis
People with compensated cirrhosis may live many years without realising that their liver is scarred. There are still enough healthy cells to keep up with the body’s needs.
But the liver gradually gets harder and harder. Eventually, blood can’t flow into the liver properly from its main blood vessel, the portal vein, because the liver is too hard. The few remaining healthy liver cells get overwhelmed.
Then you may notice symptoms like:
- Low energy
- Poor appetite
- Weight and muscle loss
- Depressed mood
- Itching
- Loss of sexual function
Decompensated cirrhosis
Decompensated cirrhosis is when you develop major complications. This is because your liver function is getting worse and there is increasing pressure in the portal vein.
Having decompensated cirrhosis is a sign that you will need to work closely with your healthcare team to manage your symptoms, improve your liver function and prevent further major complications. Your healthcare team may also suggest you be assessed for a liver transplant.
Portal hypertension
When blood can’t flow into the liver properly, pressure builds up in the portal vein system. To relieve pressure in the portal vein system, the blood takes detours around the liver in other veins in the oesophagus (food pipe) or stomach. The spleen may get larger.
This condition can lead to swelling of the belly (ascites) as fluid leaks out of the liver, or swelling in other veins (varices). When veins get swollen they can burst and bleed, which can be life threatening.
Varices
The varices – new veins in the oesophagus or stomach – can become large and may burst due to the high blood pressure and thin vessel walls, causing bleeding in the upper stomach or oesophagus.
Ascites
In decompensated cirrhosis, fluid can build up in your belly (called ascites) or chest, legs and feet (called pleural effusion). This can lead to swelling of the belly, or feeling short of breath.
Enlarged spleen
One of the jobs of the spleen is to control the number of platelets you have in your body. Platelets help your blood to clot. When the spleen gets bigger, the number of platelets in your blood may drop. This can be found in a blood test. If your platelet count is low, you may notice you bruise more easily, or it takes longer to stop bleeding if you hurt yourself.
Hepatic encephalopathy
Advanced cirrhosis can lead to confusion, called hepatic encephalopathy (HE). This is because the liver can’t remove toxins (poisons) from the blood properly. The toxins build up in the brain.
Early signs that toxins are building up in the brain may include neglecting how you look, forgetting, problems with concentration, changes in sleeping habits, or falling a lot. Severe HE can lead to confusion, disorientation or even unconsciousness (coma).
Read more about hepatic encephalopathy
Jaundice
Yellowing of the skin and the whites of the eyes (jaundice) may happen in decompensated cirrhosis.
Liver cancer
Cirrhosis of the liver is the greatest risk factor for developing liver cancer, although liver cancer can also develop in people with liver disease without cirrhosis.
Hepatocellular Carcinoma (HCC) is the commonest form of cancer that happens in people with cirrhosis. It starts in the main type of liver cells, called hepatocytes. The cells start to mutate and divide out of control. The cancer grows as lumps (tumours) throughout the liver and can eventually spread to other parts of the body.
Early diagnosis of HCC can dramatically improve the chance of having effective treatment and potentially curing the cancer. Anyone with a diagnosis of cirrhosis is recommended to have regular screening tests for liver cancer.
Read more about liver cancer (HCC)
Read more about the symptoms of liver diseaseHow is cirrhosis diagnosed?
If your doctor thinks you may have cirrhosis, they may run some tests:
- Blood tests: Liver function blood tests look for abnormal levels of liver enzymes in your blood. A full blood count can reveal a low platelet count
- Imaging: An ultrasound, contrast CT or MRI may be used to have a look at the liver structure, the size of the spleen, and to exclude any lumps that might be cancer
- Transient elastography (also known as Fibroscan or elastography): This test measures how stiff or hard the liver is
- Liver biopsy: A small sample of tissue is removed to be looked at under the microscope. This is the best way to know for certain whether you have liver cirrhosis but is not always needed
Why did I develop cirrhosis?
Cirrhosis is the result of long-term liver damage.
There are many things that can cause damage to the liver, such as too much fat build-up, unhealthy alcohol drinking, viruses, autoimmune conditions or genetic disorders. When liver damage is severe, the liver may not function normally or develop cancer.
Many people think you only get cirrhosis from drinking too much alcohol. But anything that causes progressive liver damage can lead to cirrhosis. Some other causes include:
- infection with a virus such as hepatitis B or hepatitis C
- metabolic dysfunction – problems with the metabolism that can happen when you have overweight or obesity, diabetes, poor diet or not enough exercise
- an autoimmune condition such as autoimmune hepatitis, primary sclerosing cholangitis or primary biliary cholangitis
- an inherited or genetic disease such as haemochromatosis or Wilson’s disease, alpha-1-antitrypsin deficiency, galactosemia and glycogen storage disorders
- severe reactions to prescription or over-the-counter drugs or long-term exposure to environmental toxins
- severe heart disease that leads to liver congestion.
Biliary atresia, a condition caused by absent or injured bile ducts, is the most common cause of cirrhosis in babies.
How is cirrhosis treated?
The aim of treatment is to stop or delay the disease from getting worse, prevent further damage to the liver cells, and manage and reduce complications.
Because there can be many causes of cirrhosis, your treatment plan will depend on your individual condition.
Address the cause
If the cirrhosis was caused by alcohol, it is essential to stop drinking to stop your liver damage getting worse and to allow it to heal. As any alcohol may contribute to liver injury, it is recommended to stop drinking alcohol if you have a diagnosis of cirrhosis.
If the cirrhosis was caused by viral hepatitis (hepatitis B or hepatitis C), you will be given antiviral medicines.
If you have hepatitis B cirrhosis, you will need to take these medicines your whole life. If you have hepatitis C cirrhosis, a short course of antiviral medication will clear the infection in almost everyone.
These treatments aim to remove the underlying cause of cirrhosis and may make you feel better. Treating the underlying cause reduces the risk of developing liver failure or liver cancer.
The following are usually recommended for everyone with a diagnosis of cirrhosis:
- check-ups every 6 months, including a liver ultrasound and blood tests, to monitor your liver health and check for cancer
- vaccinations against hepatitis A and B
- vaccinations against Covid-19, influenza and pneumococcus
- not drinking alcohol
- quitting smoking
Healthy lifestyle
Paying attention to nutrition is also important for people with cirrhosis to protect the liver. This factsheet on Diet for Advanced Liver Disease is a useful guide.
For example, it’s important to cut down on salt if you have fluid retention. If you are losing muscle, eating more protein is recommended. An accredited dietitian can give you an eating guide developed especially for your needs.
Medications
Medicines may be used to control the symptoms of cirrhosis. For instance, medicines called diuretics are used to remove excess fluid and to prevent oedema (swelling) and ascites from coming back.
Other medicines may be used to treat or prevent confusion or reduce the risk of developing ascites or internal bleeding. It is important to take all medicines as recommended by your doctor.
As some medicines are cleared by the liver, or may be toxic to the liver or kidneys, you may need to have your prescriptions adjusted. Always speak to your doctor first before changing your medication.
Read more about the liver and medicinesTreating complications
If your healthcare team find you have liver cancer, you will be referred to a liver specialist or multidisciplinary team to look after you. Many effective treatments are available for liver cancer as long as your liver function is still good. The earlier the diagnosis, the higher the chances of a cure.
If you develop bleeding from varices, you will be admitted urgently to hospital. You will have blood tests, fluid and medication given through a vein in your arm and possibly a blood transfusion.
You will have an endoscopy procedure. This involves a flexible tube with a camera going in through the mouth and food pipe so that rubber bands can be placed around the varices to stop them bleeding. This procedure is successful in most cases. You should be discharged from hospital on a medication called a beta-blocker, to reduce the risk of further bleeding.
In late-stage decompensated cirrhosis, a liver transplant can be a life-saving procedure. But a liver transplant isn’t always necessary or a suitable option.
Muscle cramps
Muscle cramps are a common symptom in people with cirrhosis. They are often very painful and interfere with sleep and quality of life. While cramps often affect the hands, legs and feet, they may also affect the neck, back and sides.
Cramps often become more of a problem as liver disease gets worse. They can happen more often and be more painful in people who are taking fluid tablets (diuretics) for treatment of excess body fluid.
Many treatments have been tried to reduce the intensity of muscle cramps and how often you get them. They include:
- Magnesium and/or zinc supplements. These may help some people, but many do not see a benefit
- Eating a good diet with the right amount of protein and energy intake
- A branch-chain amino acid supplement, particularly if you have muscle wasting, low albumin levels and hepatic encephalopathy (confusion that occurs in liver disease)
- Taurine, an amino-acid. This has been shown to be safe and effective to reduce the incidence, frequency and intensity of cramps. Taurine can be purchased as a powder (mixed with food or fluid), or as tablets. It is often easiest to purchase it online. The recommended dose is 1000mg twice a day.
Read more about liver treatments
More Information
If you would like to read more about cirrhosis, please download our guide.
What next?
Read more about living well Read more about living with cirrhosis
References
Bethea ED, Chopra S. Chapter 11: Cirrhosis and Portal Hypertension. In: Friedman LS, Martin PMD. (2018). Handbook of Liver Disease (4th edition). Elsevier, pp 158–171.
Brunt EM, Wong VW, Nobili V, Day CP, Sookoian S, Maher JJ, Bugianesi E, Sirlin CB, Neuschwander-Tetri BA, Rinella ME. Nonalcoholic fatty liver disease. Nat Rev Dis Primers. 2015 Dec 17;1:15080. doi: 10.1038/nrdp.2015.80. PMID: 27188459.8.
Eslam M, Sarin SK, Wong VW, Fan JG, Kawaguchi T, Ahn SH, Zheng MH, Shiha G, Yilmaz Y, Gani R, Alam S, Dan YY, Kao JH, Hamid S, Cua IH, Chan WK, Payawal D, Tan SS, Tanwandee T, Adams LA, Kumar M, Omata M, George J. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol Int. 2020 Dec;14(6):889-919. doi: 10.1007/s12072-020-10094-2.
de Lédinghen V, Vergniol J. Transient elastography (FibroScan). Gastroenterol Clin Biol. 2008 Sep;32(6 Suppl 1):58-67. doi: 10.1016/S0399-8320(08)73994-0.
Iser D, Marno R. Fatty liver disease A practical guide for GPs. Aust Fam Physician 2013;42:444–447.
Hepatocellular Carcinoma Consensus Statement Working Group. Australian recommendations for the management of hepatocellular carcinoma: a consensus statement. Melbourne: Gastroenterological Society of Australia, 2020.
Schmeltzer PA, Russo MW (2019). Chapter 13: General Care of the Cirrhotic Patient. In: Cohen SM, Davitkov P (eds). Liver Disease: a Clinical Casebook. Springer, pp 165–177.
The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017 Lancet Gastroenterol Hepatol 2020;5:245–266.
Tsochatzis EA, Bosch J, Burroughs AK. Liver cirrhosis. Lancet. 2014 May 17;383(9930):1749-61. doi: 10.1016/S0140-6736(14)60121-5. Epub 2014 Jan 28.
Reviewed June 2025